I’m often asked by people concerned about the impending increase in individuals who may demand health care, “where are all these all of them going to go?” I have no crystal ball, and obviously the answer will vary by population, but the short answer is that many of them will seek care in federally qualified health centers: A federally qualified health center (FQHC) is a type of provider defined by the Medicare and Medicaid statutes. FQHCs include all organizations receiving grants under Section 330 of the Public Health Service Act, certain tribal organizations, and FQHC Look-Alikes. Requirements for Indian Health Service funded FQHCs may differ from the requirements for FQHCs receiving Section 330 grants and for FQHC Look-Alikes. There are lots of benefits to being a FQHC. These include: For new starts, funding up to $650,000 can be requested. Other benefits include:
- Cost-based reimbursement for services provided under Medicare
- Reimbursement under the Prospective Payment System (PPS) or other State-approved Alternative Payment Methodology (APM) for services provided under Medicaid
- Medical malpractice coverage through the Federal Tort Claims Act
- Eligibility to purchase prescription and non-prescription medications for outpatients at reduced cost through the 340B Drug Pricing Program
- Access to National Health Service Corps
- Access to the Vaccine for Children Program
- Eligibility for various other federal grants and programs
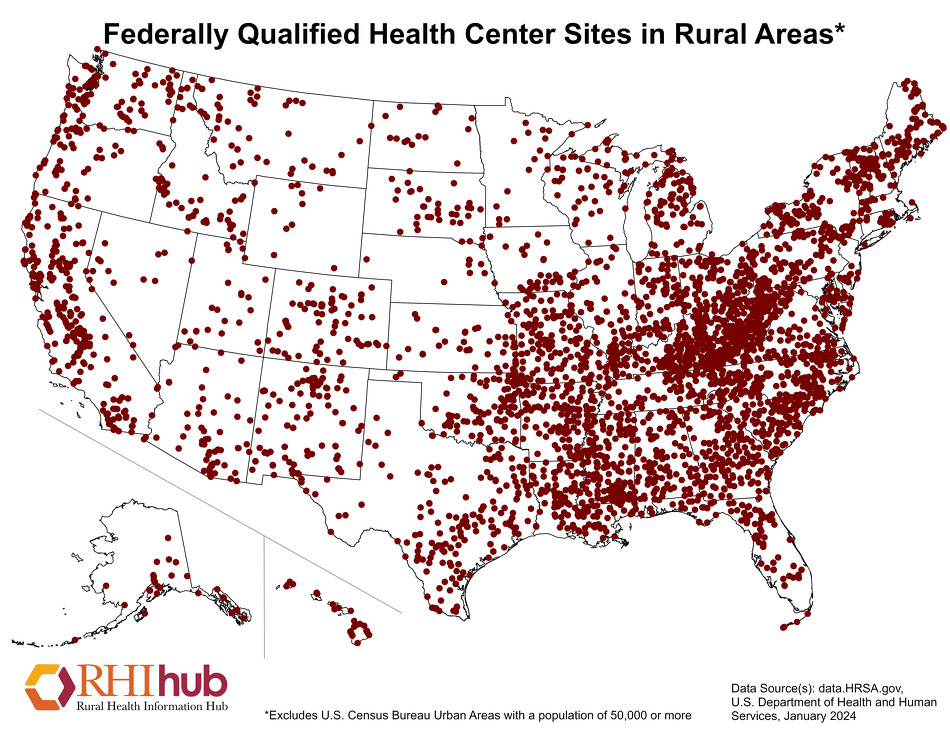
These centers were mostly established back in 1991 under the first President Bush. The second, and more recent of the Bush Presidents, significantly expanded their use, as did President Obama under the Affordable care Act. It’s thought that 30 million or so Americans might be receiving health care through organizations such as these in the future. They’re much more common than you might think:
{kind=link}

Background: The 2010 Affordable Care Act relies on Federally Qualified Health Centers (FQHCs) and FQHC look-alikes (look-alikes) to provide care for newly insured patients, but ties increased funding to demonstrated quality and efficiency.
Purpose: To compare FQHC and look-alike physician performance with private practice primary care physicians (PCPs) on ambulatory care quality measures.
Methods: The study was a cross-sectional analysis of visits in the 2006–2008 National Ambulatory Medical Care Survey. Performance of FQHCs and look-alikes on 18 quality measures was compared with private practice PCPs. Data analysis was completed in 2011.
Basically, this study looked at national-level data to compare how FQHC’s compared to private practices with respect to 18 different quality measures. What did they find? On eleven of the measures, there was no difference between the two groups; FQHC’s were equal to their private practice counterparts. On one (diet counseling for at-risk adolescents), they did slightly worse. But on the remaining six, they outperformed private practices. FQHC’s were superior at using ACE inhibitors for congestive heart failure. They were better at using aspirin for coronary heart disease. They were also better at using beta-blockers for coronary artery disease, at not using benzodiazepines for depression, at screening for blood pressure, and at not using screening EKGs in low-risk populations. But that was the unadjusted analysis. Once the researchers adjusted for patient characteristics, private practices no longer were better than FQHCs on any metrics at all. I know this will surprise many who are inclined to believe that the government is bad at everything. But in this case, the research indicates that’s just not true. It’s also not true with respect to VA medical centers, which often do better than the private sector in terms of quality. But that’s for another blog post. FQHC’s are likely going to expand in the coming years. They will often be asked to pick up the slack in terms of seeing the newly insured, especially those who are getting Medicaid through the expansion of the program. That’s not a bad thing. -Aaron Dr. Aaron E. Carroll is an associate professor and vice chair of health policy and outcomes research in the department of pediatrics at the Indiana University School of Medicine. He blogs about health policy at The Incidental Economist and tweets at @aaronecarroll. As part of our ongoing effort to raise awareness of health services research and increase its application in policy and practice, AcademyHealth has partnered with Austin Frakt, Ph.D., and Aaron Carroll, M.D., M.S., to contribute posts on the subjects of health care costs, delivery system transformation, and public and population health – areas AcademyHealth has identified as a priority in the current policy environment. As regular contributors, they’ll be discussing current events with an eye toward how new and existing research informs the issues